
04 Aug The 10 Biggest Learning Science Breakthroughs and the Implications for Medical Simulation Training
A recent blog post, “The 10 Biggest Breakthroughs in the Science of Learning” sparked an animated discussion here about the design and effectiveness of medical training. It raised some compelling questions. How do these principles apply to medical simulation training? What gamification elements will work best in a medical setting? How does stress affect learning? How do millennials prefer to learn? There is easily enough material for an eBook, but meanwhile here are the 10 principles and how we use them in medical simulation training.
1. More Information doesn’t mean more learning
Our brains can only take so much. When too much information is delivered simultaneously we experience cognitive overload. It has been shown the students are unlikely to learn or recall information when too much is delivered at one time. There are several methods of avoiding cognitive overload: chunking, schemas, associating with a real experience and combining visual and auditory experience.
Perioperative nurses entering the OR for the first time are faced with trying to absorb a lengthy sequence of steps, a huge variety of instruments and an instrument handling protocol — all in the stressful environment of a surgery. We can avoid cognitive overload with simulation training before nurses enter the OR. Surgeries are broken down step by step. Associating with a real experience is achieved by using real surgical video. Using narration and interactive video brings together auditory and visual learning. Finally integrating instrument recognition within a real surgery helps students build a mental schema for structuring the information.
2. The brain is a highly dynamic organ
Our brains get re-wired throughout our lives. Its called neuroplasticity. Until very recently, it was assumed that the brain remained static after a certain stage of childhood. It is now known that the brain changes through adulthood in response to experience, both in structure and functional organization. Synaptic pruning is the principle that neurons are recreated and removed depending on how they are used. Neurons that fire simultaneously will become part of the same cortical map (area of the cortex).
When a stimulus is reinforced the corresponding area of the cortex gets larger and stronger. Stimuli associated with rewards show the greatest changes. Neuroplasticity effects are far quicker than expected. A study looking at the brains of medical students studying for their finals showed changes in the size of the cortex in just a few months. Positive reinforcement, repetition and rewards are fundamental elements of gamification, with direct effects on neuroplasticity. We are only just scratching the surface of how this can be applied to training, brain injuries and age-related cognitive decline.
3. Emotion influences the ability to learn
We are emotional learners. When we are stressed or humiliated, we struggle to learn. Our limbic system kicks in, inhibiting learning, memory and higher level processing. Conversely when we are in a positive learning environment more information is passed into the higher functioning area of the prefrontal cortex.
It’s not just in the classroom. The OR can be a stressful environment, where hesitation and mistakes are just not acceptable. Anxiety before entering the OR can lead to errors, which sets up a negative cycle of stress and learning inhibition.
By enabling nurses to practice safely before entering the OR, we allow them to learn in a safe, stress-free environment, building confidence and mastery. Gamification rewards learning with a trickle of small wins, building a positive reinforcement loop that encourages students to move to the next stage. Scoring helps learners track their own progress and motivates them to hone their skills. Leaderboards mean learners can rate their skills relative to others in their field (privately or publicly). By providing an engaging, safe learning environment, we can equip nurses with the knowledge they will need to recall accurately in the stressful OR environment.
4. Mistakes are an essential part of learning
Your training wheels must come off — and you will fall. Mastery of any skill, from learning to walk to assisting a surgery, will involve mistakes. Failure is a necessary part of learning and yet we continually create scenarios, both in school and work, where the stakes are high and mistakes are penalized. Learning Science advises a ‘no penalty’ mode, where learners are only rewarded for successes, but never penalized for errors. Simulation training with gamification elements means we can reward every small success, focusing on and reinforcing correct responses. Students move through errors, never losing points but always having the chance to correct their responses and move ahead. The decision to repeat the simulation and get a higher score is one motivated by confidence that the skills can be honed.
5. The brain needs novelty
Novelty stokes our dopamine. Not only does that make us feel good but it prompts the brain to engage and learn more about the novel stimuli. Dopamine is a neurotransmitter that not only produces pleasure but also helps with perseverance and resilience to setbacks. Rote learning, textbooks and flashcards are dull and repetitive. Nurses and medical students have been learning from flashcards for decades. Zero novelty. Zero motivation. Gamified simulations challenge learners, motivate progress towards a goal and reward success. Adding in a timing dimension pushes learners to stay engaged and complete the task on time. Scoring rewards the learner throughout the simulation and provides a tangible metric for measuring personal success. Gaining small rewards throughout the simulation, learners are motivated to repeat the challenge and improve their scores. That’s addictive.
6. There are no learning styles

Forget the labels – you are not a kinesthetic learner! It turns out that the many different models for learning put forward over the years are nowhere near as important as simply accommodating individual students’ abilities, preferences, social and emotional needs. Every individual will respond to a different mix of auditory, visual, kinesthetic and other learning models. An ideal learning environment will combine these modes in a stimulating, positive way. iPad based simulation training using voice prompts, video and simple gestures engages the learner with multiple stimuli. VR simulation goes even further, adding full spatial awareness and requiring accurate gestures.
7. Brains operate on the use it or lose it principle
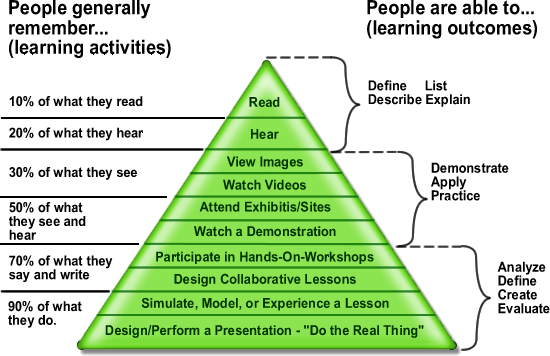
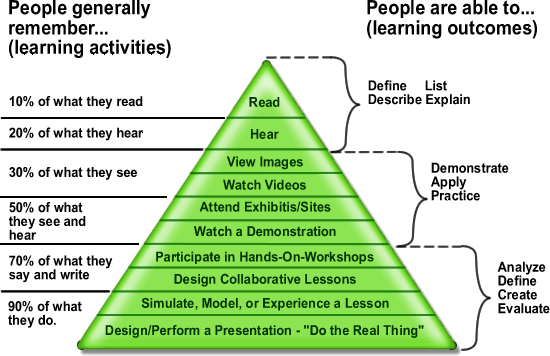
You may remember some fragments of your school geometry theorems but most people fail to retain information that is not regularly used. Neural pathways need regular chemical and electrical stimulation to survive — otherwise they will be lost. After just 2 weeks we will only remember 10% of what we read, 20% of what we hear, 30% of what we see, 50% of what we see and hear, 70% of what we say and 90% of what we say and do. Edgar Dale’s Cone of Learning has been a guiding principle for instructional design since the late sixties. He also divides learning into active and passive modes. Simulation falls into the top tier of the active category — we learn best by doing the real thing or simulating it.
Long term retention rates are also an issue in a clinical setting. When designing our simulation app for perioperative nurses we focused initially on student scrub nurses. We quickly realized that highly experienced nurses scrubbing into a procedure they hadn’t done for years (or a new specialty) were equally important. They told us that this is a significant source of stress and anxiety in their roles. They needed a way to refresh their knowledge of the procedure and instruments beforehand. Being able to practice on an iPad simulation app at home or in the hospital means that they can go into the surgery more confident and more proficient.
8. Learning is social
Babies learn from their mothers’ smiles — it’s our first social cue. Right from infancy, learning is spurred by social cues. People learn better when they recall or emulate the actions or words of another person. We learn by seeing and hearing other people — whether live or online — whether real or virtual. Peer collaboration engages students in a social context and stimulates multiple senses: talking, hearing, seeing, moving — all of which help with longer term retention.
Multi-player VR simulation takes this a step further, enabling people to learn collaboratively, in a realistic version of their working environment. For surgical teams, this could have huge practical benefits, just as it has in the aviation industry. Teams need to learn how to deal with unexpected, adverse circumstances such as an emergency code over the PA or dropping a pan. These real-life variables are very hard to train for. This is where simulation really comes into its own.
The term social learning is also increasingly applied to learning through social media tools – collaborating, discussing and blogging to stimulate learning as a group.
9. Learning is best when innate abilities are capitalized on
We seem to have innate capabilities to recognize patterns, mirror actions and learn languages. The more we can harness these innate abilities, the easier it will be to learn a new concept. When encountering new information, our brains try to integrate and sort the new information. We have mental schemas, which are mental frameworks of preconceived ideas. We are much more likely to pay attention to and absorb new concepts and details that fit with pre-existing schemas.
In designing training, the more that we can teach patterns rather than discrete details, the easier it will be for learners to retain. Contrast learning a pile of individual instrument flashcards to learning within the context of a surgery. Consulting with preoperative educators we were also advised to teach the meta-level patterns for surgery that repeat within most surgeries. This is another example of learning to recognize patterns.
10. Learning can change brain structure
As we become expert in a specific area, our brain actually changes. It is mostly at the synapse level, making new connections and strengthening existing connections but can actually change the shape of the brain. London taxi drivers were found to have a larger hippocampus than bus drivers due to the huge amount of spatial information they have to retain and constantly use compared to bus drivers following limited set routes. Similarly bilingual people have a larger left parietal cortex and professional musicians have increased cortex volume. It seems that if we stimulate multiple senses during learning we activate more neural pathways and sometimes reinforce the same pathway simultaneously.
If we can harness simulation to engage multiple learning modes and provide a positive, motivational learning environment, the better the learning outcomes and retention rates of our students. In the surgical setting that means staff are less stressed, better prepared and patient outcomes are improved.